Tibia (Shinbone) Shaft Fractures
The tibia, or shinbone, is the most common fractured long bone in your body. The long bones include the femur, humerus, tibia, and fibula. A tibial shaft fracture occurs along the length of the bone, below the knee and above the ankle.
Because it typically takes a major force to break a long bone, other injuries often occur with these types of fractures.
AnatomyThe lower leg is made up of two bones: the tibia and fibula. The tibia is the larger of the two bones. It supports most of your weight and is an important part of both the knee joint and ankle joint.
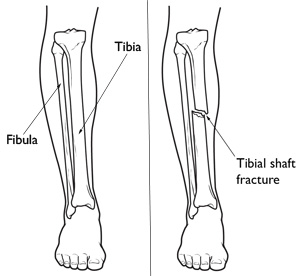 The tibia is the larger bone in your lower leg. Tibial shaft fractures occur along the length of the bone.
Types of Tibial Shaft Fractures
The tibia is the larger bone in your lower leg. Tibial shaft fractures occur along the length of the bone.
Types of Tibial Shaft Fractures
The tibia can break in several ways. The severity of the fracture usually depends on the amount of force that caused the break. The fibula is often broken as well.
Common types of tibial fractures include:
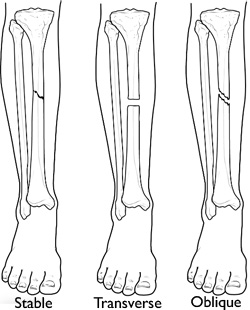
Stable fracture: This type of fracture is barely out of place. The broken ends of the bones basically line up correctly and are aligned. In a stable fracture, the bones usually stay in place during healing.
Displaced fracture: When a bone breaks and is displaced, the broken ends are separated and do not line up. These types of fractures often require surgery to put the pieces back together.
Transverse fracture: This type of fracture has a horizontal fracture line. This fracture can be unstable, especially if the fibula is also broken.
Oblique fracture: This type of fracture has an angled pattern and is typically unstable. If an oblique fracture is initially stable or minimally displaced, over time it can become more out of place. This is especially true if the fibula is not broken.
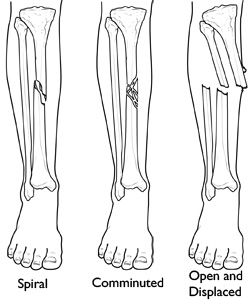
Spiral fracture: This type of fracture is caused by a twisting force. The result is a spiral-shaped fracture line about the bone, like a staircase. Spiral fractures can be displaced or stable, depending on how much force causes the fracture.
Comminuted fracture: This type of fracture is very unstable. The bone shatters into three or more pieces.
Open fracture: When broken bones break through the skin, they are called open or compound fractures. For example, when a pedestrian is struck by the bumper of a moving car, the broken tibia may protrude through a tear in the skin and other soft tissues.
Open fractures often involve much more damage to the surrounding muscles, tendons, and ligaments. They have a higher risk for complications and take a longer time to heal.
Closed fracture: With this injury, the broken bones do not break the skin. Although the skin is not broken, internal soft tissues can still be badly damaged. In extreme cases, excessive swelling may cut off blood supply and lead to muscle death, and in rare cases, amputation.
CauseHigh-energy collisions, such as an automobile or motorcycle crash, are common causes of tibial shaft fractures. In cases like these, the bone can be broken into several pieces (comminuted fracture).
Sports injuries, such as a fall while skiing or running into another player during soccer, are lower-energy injuries that can cause tibial shaft fractures. These fractures are typically caused by a twisting force and result in an oblique or spiral type of fracture.
SymptomsThe most common symptoms of a tibial shaft fracture are:
- Pain
- Inability to walk or bear weight on the leg
- Deformity or instability of the leg
- Bone "tenting" the skin or protruding through a break in the skin
- Occasional loss of feeling in the foot
It is important that your doctor knows the circumstances of your injury. For example, if you fell from a tree, how far did you fall? It is just as important for your doctor to know if you sustained any other injuries and if you have any other medical problems, such as diabetes. Your doctor also needs to know if you take any medications.
After discussing your symptoms and medical history, your doctor will do a careful examination. He or she will assess your overall condition, and then focus on your leg. Your doctor will look for:
- Obvious deformity such as angulation or shortening (the legs are not the same length)
- Breaks in the skin
- Contusions (bruises)
- Swelling
- Bony prominences under the skin
- Instability (some patients may retain a degree of stability if the fibula remains intact or the fracture is incomplete)
After the visual inspection, your doctor will feel along your leg to see if there are abnormalities of the tibia. If you are awake and alert, your doctor will test your sensation and muscle strength by asking you to move your toes and see if you can feel different areas over your foot and ankle.
TestsOther tests that may help your doctor confirm your fracture include:
X-rays
X-rays can show if the bone is broken and whether there is displacement (the gap between broken bones). They can also show how many pieces of bone there are. X-rays are also useful for identifying the involvement of the knee or ankle joint, and the presence of a fibula fracture.
Computed tomography (CT) scan
After reviewing your x-rays, your doctor may recommend a CT scan of your leg. This is often done if there is a question of the fracture extending into either the knee or ankle joint. A CT scan shows a cross-sectional image of your limb. It can provide your doctor with valuable information about the severity of the fracture.
TreatmentIn planning your treatment, your doctor will consider several things, including:
- The cause of your injury
- Your overall health
- The severity of your injury
- The extent of soft tissue damage
Nonsurgical Treatment
Nonsurgical treatment may be recommended for patients who:
- Are poor surgical candidates due to their overall health problems
- Are less active, so are better able to tolerate small degrees of angulation or differences in leg length
- Have closed fractures with only two major bone fragments and little displacement (gap)
Initial treatment. Most injuries cause some swelling for the first few weeks. Your doctor may initially apply a splint to provide comfort and support. Unlike a full cast, a splint can be tightened or loosened, and allows swelling to occur safely. Once the swelling goes down, your doctor will consider a range of treatment options.
Cast and functional brace. One proven nonsurgical treatment method is to immobilize the fracture in a cast for initial healing. After weeks in the cast, it can be replaced with a functional brace made of plastic and fasteners. The brace will provide protection and support until healing is complete. The brace allows you to take it off for hygiene issues and for physical therapy.
Surgical Treatment
Your doctor may recommend surgery for your fracture if it is:
- An open fracture with wounds that need monitoring
- Extremely unstable because of many bone fragments and large degrees of displacement
- Not healed with nonsurgical methods
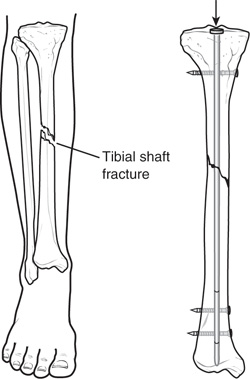
Intramedullary nailing. The current most popular form of surgical treatment for tibial fractures is intramedullary nailing. During this procedure, a specially designed metal rod is inserted from the front of the knee down into the marrow canal of the tibia. The rod passes across the fracture to keep it in position.
 Intramedullary nailing.
Intramedullary nailing.
Intramedullary nails come in various lengths and diameters to fit most tibia bones. The intramedullary nail is screwed to the bone at both ends. This keeps the nail and the bone in proper position during healing.
Intramedullary nailing allows for strong, stable, full-length fixation. The technique also makes it more likely that the position of the bone obtained at the time of surgery will be maintained when compared with casting or external fixation.
Intramedullary nailing is not ideal for fractures in children and adolescents because care must be taken to avoid crossing the bone's growth plates.
Plates and screws. Tibial shaft fractures were once routinely treated with plate and screw constructs. These tools are reserved for fractures in which intramedullary nailing may not be possible or optimal, such as certain fractures that extend into either the knee or ankle joints.
During this type of procedure, the bone fragments are first repositioned (reduced) into their normal alignment. They are held together with special screws and metal plates attached to the outer surface of the bone.
External fixation. In this type of operation, metal pins or screws are placed into the bone above and below the fracture site. The pins and screws are attached to a bar outside the skin. This device is a stabilizing frame that holds the bones in the proper position so they can heal.
While external fixation has yielded some reasonable results, having implants outside the body has proven to be somewhat unpopular with many patients and physicians.
RecoveryHow long it takes to return to daily activities varies with different types of fractures. Some tibial shaft fractures heal within 4 months, yet many may take 6 months or longer to heal. This is particularly true with open fractures and fractures in patients who are less healthy.
- Early motion. Many doctors encourage leg motion early in the recovery period. For example, if soft tissue injury is present with a fracture, the knee, ankle, foot, and toes may be mobilized early in order to prevent stiffness.
- Physical therapy. While you are wearing your cast or splint, you will likely lose muscle strength in the injured area. Exercises during the healing process and after your cast is removed are important. They will help you restore normal muscle strength, joint motion, and flexibility.
- Weightbearing. When you begin walking, you will most likely need to use crutches or a walker.
It is very important to follow your doctor's instructions for putting weight on your injured leg to avoid problems. In some cases, doctors will allow patients to put as much as weight as possible on the leg right after surgery. However, you should always follow the specific directions given by your surgeon.
Fracture pain usually stops long before the bone is solid enough to handle the stresses of everyday activities. If the bone is not healed and you put weight on it too soon, it could fail to heal. If that occurs, you may need a secondary surgical procedure, such as bone grafting or revision fixation.
ComplicationsA tibial shaft fracture can cause further injury and complications.
- Sharp fragments may cut or tear adjacent muscles, nerves, or blood vessels.
- Excessive swelling may lead to compartment syndrome, a condition in which the swelling cuts off blood supply to the leg. This can result in severe consequences and requires emergency surgery once it is diagnosed.
- Open fractures can result in long-term deep bony infection or osteomyelitis, although prevention of infection has improved dramatically over the past generation.
Surgical Complications
Surgical complications include:
- Malalignment, or the inability to correctly position the broken fragments
- Infection
- Nerve injury
- Vascular injury
- Blood clots (these may also occur without surgery)
- Nonunion (failure of bone to heal)
- Angulation (with treatment by external fixation)
Secondary Surgery
Certain factors are often associated with difficulties in fracture healing. Open fractures, in which the bone fragments are displaced enough to exit the skin, typically sustain greater injury and are at increased risk for infection. This may stall or prevent healing. These fractures are more likely to require secondary surgical procedures.
Fractures that are directed straight across the bone are typically the result of higher energy mechanisms (as opposed to the spiral-type fractures seen with low-energy twisting injuries). They also have increased injury to the tissues that are required for healing, and are associated with a greater occurrence of secondary surgeries.
These two factors are beyond the surgeon's control. A third and more controllable factor is getting the major fragments in line with each other and pushed together with surgery.
In addition, your general health may have an effect on healing. Smoking and corticosteroid use affect both bone and skin healing, so it is important to tell your doctor if you use these.
ResearchBone morphogenetic proteins (BMPs) make up a new class of proteins that has been identified with factors that promote bone healing. Some of these proteins have been isolated and are now available for use as adjuncts to healing. Studies are ongoing to determine the ultimate value of these proteins, but early reports have been favorable.
If you found this article helpful, you may also be interested in Fractures of the Proximal Tibia (Shinbone).
Source: http://orthoinfo.aaos.org/topic.cfm?topic=A00522