Elbow Fractures in Children
Information on elbow fractures in children is also available in Spanish: Fracturas de los codos en los niños.
Elbow fractures are common childhood injuries, accounting for about 10% of all childhood fractures. In many cases, a simple fracture will heal well with conservative cast treatment. Some types of elbow fractures, however, including those in which the pieces of bone are significantly out of place, may require surgery. Other structures in the elbow—such as nerves, blood vessels, and ligaments—may also be injured when a fracture occurs and require treatment, as well.
Anatomy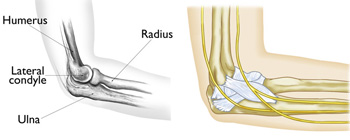 (Left) The main bones of the elbow, when viewed from the side. (Right) The major nerves and ligaments are highlighted.
(Left) The main bones of the elbow, when viewed from the side. (Right) The major nerves and ligaments are highlighted.
The elbow is a joint made up of three bones—the humerus, radius, and ulna.
- The humerus is the upper arm bone between the shoulder and the elbow.
- The radius is one of the forearm bones between the elbow and wrist. The radius is on the "thumb side" of the forearm.
- The ulna is the other forearm bone between the elbow and wrist, running next to the radius. The ulna is on the "pinky finger side" of the forearm.
Ligaments on the inner and outer sides of the elbow hold the joint together and muscles surround the joint on the front and back sides. The elbow joint is crossed by three major nerves.
DescriptionThere are several types of elbow fractures, including:
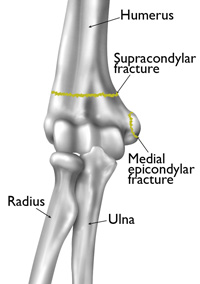 Common childhood elbow fractures include supracondylar fractures and medial epicondylar fractures.
Reproduced and adapted from J Bernstein, ed: Musculoskeletal Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003.
Common childhood elbow fractures include supracondylar fractures and medial epicondylar fractures.
Reproduced and adapted from J Bernstein, ed: Musculoskeletal Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003.
Above the elbow (supracondylar). In this type of fracture, the upper arm bone (humerus) breaks slightly above the elbow. These fractures usually occur in children younger than eight years old. This is the most common type of elbow fracture, and one of the more serious because it can result in nerve damage and impaired circulation.
At the elbow knob (condylar). This type of fracture occurs through one of the bony knobs (condyles) at the end of the upper arm bone. Most occur through the outer, or lateral, knob. These fractures require careful treatment, because they can disrupt both the growth plate (physis) and the joint surface.
At the inside of the elbow tip (epicondylar). At the top of each bony knob is a projection called the epicondyle. Fractures at this point usually occur on the inside, or medial, epicondyle in children from 9 to14 years of age.
Growth plate (physis). The upper arm bone and both forearm bones have areas of cartilage called growth plates located near the end of the bone. Because growth plates help determine the length and shape of the mature bone, a fracture that disrupts the growth plate can result in arrested growth and/or deformity if not treated promptly.
Forearm. An elbow dislocation can break off the head of the radius bone, and excessive force can cause a compression fracture to the radius, as well. Fractures of the tip (olecranon) of the ulna are rare.
Fracture dislocation. A fracture of the ulna associated with a dislocation of the top of the radius at the elbow is called a Monteggia fracture. If the dislocation is not recognized, and only the fracture is treated, it can lead to permanent impairment of elbow joint function.
Open fracture. When a broken bone breaks through the skin, it is called an open fracture. An open fracture often involves damage to the muscles, tendons, and ligaments and takes a longer time to heal.
CauseIn most cases, elbow fractures in children are caused by:
- A fall on an outstretched arm
- A fall directly on the elbow
- A direct blow to the elbow
Children regularly engage in many activities that put them at risk for injuries to the elbow. Many elbow injuries occur on the playground when children lose their grip on the monkey bars or other equipment. For toddlers, a fall from a lower height can cause an elbow fracture. Elbow fractures may also occur in sports, such as gymnastics or football, or recreational activities such as skateboarding or bicycling.
Wearing protective elbow guards and pads can help reduce the risk of a fracture about the elbow.
SymptomsNo matter where the break occurs, most elbow fractures result in sudden, intense pain in the elbow and forearm. Other common symptoms include:
- Swelling around the elbow
- Numbness in the hand, a sign of potential nerve injury
- Inability to straighten the arm
If your child complains of elbow pain after a fall and refuses or is unable to move his or her arm, it is important to see a doctor immediately.
Doctor ExaminationPhysical Examination
After discussing your child's symptoms and medical history, your doctor will perform a careful examination of your child's arm to determine the extent of the injury. He or she will look for:
- Tenderness
- Swelling
- Bruising
- Limited movement
- Change in color in the hand, an indication that circulation has been affected
During the physical examination, your doctor will also check to see whether any damage to the nerves or blood vessels has occurred.
.jpg) (Left) This child has a severe fracture of the humerus above the elbow. (Right) This x-ray of the fracture shows that the humerus has broken into two parts-a complete displacement.
(Courtesy of Texas Scottish Rite Hospital for Children)
(Left) This child has a severe fracture of the humerus above the elbow. (Right) This x-ray of the fracture shows that the humerus has broken into two parts-a complete displacement.
(Courtesy of Texas Scottish Rite Hospital for Children)
X-Rays
X-rays provide clear images of dense structures such as bone. An x-ray will indicate what kind of fracture has occurred, and whether the bones have angulated or moved out of alignment (displaced). Because a child's bones are still forming, your doctor may request x-rays of both arms for comparison.
TreatmentIf an elbow fracture heals in the wrong position, the elbow may remain permanently crooked and have limited range of motion. For this reason, it is important that the fracture be treated correctly at the time of the initial injury.
Treatment for elbow fractures depends on the type of fracture and the degree of displacement.
Nonsurgical Treatment
Many stable fractures heal successfully with cast or splint immobilization. If the fracture is stable with no displacement, your doctor may directly apply a splint or cast to keep the bones in proper alignment while they heal.
Splints provide less support than casts; however, they can be easily adjusted to accommodate swelling from injuries. In many cases, a splint is applied to a fresh injury first. As swelling subsides, a full cast may replace the splint.
In some stable elbow fractures, the bones may need to be repositioned before applying a splint or cast. In this procedure—called a closed reduction—your doctor gently moves the arm to manipulate the bones back into place. Your child will be given some form of sedation or anesthesia for this procedure.
As the fracture heals, your doctor may schedule additional x-rays to make sure the bones stay in place.
.jpg) This x-ray shows a supracondylar humerus fracture that has been put into the correct position and held in place with two pins. The pins will be removed after healing has begun.
Reproduced from: Surgical management of pediatric fractures in the upper extremity, Flynn J, Sarwark J, Waters P, Bae D, Lemke L: Instr Course Lect 2003, 54: 635-645.
This x-ray shows a supracondylar humerus fracture that has been put into the correct position and held in place with two pins. The pins will be removed after healing has begun.
Reproduced from: Surgical management of pediatric fractures in the upper extremity, Flynn J, Sarwark J, Waters P, Bae D, Lemke L: Instr Course Lect 2003, 54: 635-645.
Surgical Treatment
If the bone fragments are displaced, surgery may be required to ensure that the fracture heals fully.
Closed reduction and percutaneous pinning. In this procedure, the displaced bone fragments are repositioned during closed reduction and held in place with metal pins. The pins are inserted through the skin, into the bone and across the fracture. A splint is applied to protect the area for the first week, then is typically replaced with a cast. The pins and cast are removed after healing has begun, a few weeks after surgery.
Open reduction and internal fixation. Open fractures, fractures that cannot be repositioned during a closed reduction, and fractures that are accompanied by nerve or vascular injuries require open surgery or open reduction and internal fixation.
RecoveryWhether the fracture is treated by simple immobilization or with surgery, the arm will be placed in a cast or splint for 3 to 6 weeks, depending upon the fracture.
When the fracture is well enough healed, the doctor may recommend specific exercises to improve the range of motion in the joint.
In most cases, the elbow's range of motion returns to normal, or has just a mild limitation.
Statistical data on this webpage was reviewed by the AAOS Department of Research and Scientific Affairs.
Source: http://orthoinfo.aaos.org/topic.cfm?topic=A00037